




MEN’S SEXUAL FUNCTION, ANDROPAUSE AND TESTOSTERONE
INTRODUCTION
For humans, sex and sexuality are remarkably complex. Sex serves a biological purpose, a psychological purpose and a social purpose. Many different organs and systems are involved in coordinating sexual response including the brain, the spinal chord, blood vessels, the reproductive organs and various hormones such as testosterone. Interference with any one of these factors can result in sexual problems (sexual dysfunction).
Gender
Obviously, men and women have different hormones. Men have about 10 times the testosterone in their bodies compared to women and women have about 10 times the estrogen compared to men.
But did you know that both hormones are manufactured from the body’s cholesterol? Normal cholesterol levels are important for the production of healthy hormone levels
Male Sexual Function
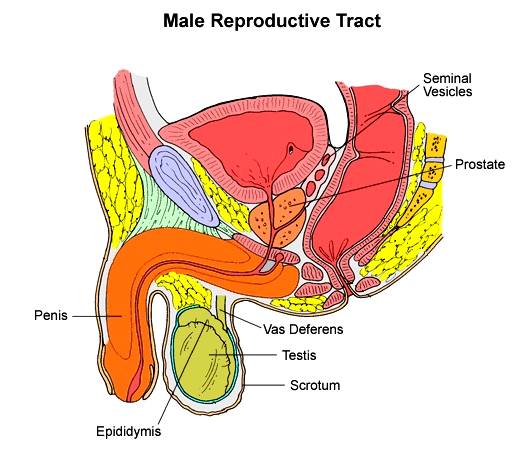
All of the male reproductive organs (Fig. 1) are regulated by testosterone and testosterone derivatives such as DHT (dihydrotestosterone) and estrogen. These include the penis, the testes (testicles), the epididymis the vas deferens, the seminal vesicles the prostate, Cowper’s gland and the ejaculatory duct. During puberty, testosterone plays a major role in the maturation, physical growth and function of the various reproductive organs. During adulthood, testosterone continues to provide a role for function and maintenance of the reproductive organs but not for growth. There are no receptors for testosterone in the adult penis for growth. As an adult, a man’s penis is as big as it is going to be 1.
A normal adult testicle is about 2.0 in long by 1.33 in wide. Ninety percent of the adult testicle is sperm producing tissue. Only 2.5% of the testicle is testosterone-producing tissue (called Leydig cells) yet this rather small amount of tissue produces 95% of a man’s testosterone. The rest of the testicle’s volume is blood vessels and connective tissue. The production of sperm requires a lot of testosterone and so the testicles produce proteins that keep testosterone concentrated in the testes. The concentration of testosterone in the testicles is over 100 times the concentration of testosterone in the blood 1.
The sperm that are ejaculated today were produced 75 days ago. Sperm make up a rather small portion of the semen that is released during ejaculation. The testicles contribute only 5% of the total volume of semen. Yet in each millilitre (1/30 ounce) of semen there are normally over 20 million sperm 1.
The volume of semen per ejaculate is from ½ to 1 teaspoon. Lower volumes may occur after very frequent ejaculation and higher volumes are seen after prolonged abstinence. Volumes consistently less than 1.5 ml (hypospermia) or more than 5.5 ml (hyperspermia) are abnormal. The purpose of semen is purely for reproduction as a vehicle to carry the sperm into the female reproductive tract. Although ejaculation of semen accompanies orgasm and sexual pleasure, erection and orgasm are controlled by separate mechanisms and semen emission is not essential for enjoyable sex in most people. Having said that, it is true that a man’s feeling of orgasmic pleasure is in part attributable to the volume of ejaculate: the greater the volume of ejaculate the more intense the orgasm.
Semen is made from the secretions of several glands and each of these glands requires testosterone support for its function. The following table shows the makeup of semen.
| Contributing gland | Percentage of whole ejaculate |
|---|---|
| Testicles and epididymes | 5 per cent |
| Seminal vesicles | 46 to 80 per cent |
| Prostate gland | 13 to 33 per cent |
| Bulbourethral (Cowper’s) and urethral glands | 2 to 5 per cent |
The following paragraphs outline the functions of other male reproductive glands.
Seminal Vesicles
The seminal vesicles usually contribute more than half of the seminal volume. Their secretions are particularly rich in a sugar called fructose, which is an essential nutrient for the sperm. They also produce a substance that causes the semen to clot (become sticky or jelly-like) after ejaculation, thought useful in reproduction for keeping the semen at the neck of a woman’s womb (cervix).
Prostate Gland
The secretions of the prostate gland contain several chemicals, of which prostate specific antigen (PSA) is probably the most important. PSA is an enzyme. The prime function of PSA is to liquefy the clotted semen, so that the sperm can escape from it and swim off to fertilise the egg in the woman’s reproductive tract. Prostate gland cells produce PSA and some of it leaks into the blood stream, as well as appearing in semen. The bigger and more active the prostate gland is, the more PSA appears in the blood. Men with big, benign (non-cancerous) prostate glands often have higher blood levels of PSA than average. Men with prostate cancer may have very high levels. However, PSA levels can also be normal in both conditions. It is a useful marker of prostate gland size and activity, but is not a specific test for prostate cancer. (For more information, follow this link to The Prostate Gland on this website).
Bulbourethral (Cowper’s) and Urethral glands
The secretions of these glands lubricate the male reproductive tract.
“Normal” Sperm
The World Health Organization provides a definition of a ‘normal’ sperm count:
- the concentration of sperm should be at least 20 million per ml.
- the total volume of semen should be at least 2ml.
- the total number of sperm in the ejaculate should be at least 40 million.
- at least 75 per cent of the sperm should be alive (it is normal for up to 25 per cent to be dead).
- at least 30 per cent of the sperm should be of normal shape and form.
- at least 25 per cent of the sperm should be swimming with rapid forward movement.
- at least 50 per cent of the sperm should be swimming forward, even if only sluggishly.
It is quite surprising how many dead and abnormal sperm can be present in a ‘normal’ sample. Sperm counts can vary tremendously from day to day. Also, with age, there is a decrease in the quality of sperm due to a reduction in the number of sperm, an increase in the number of abnormal sperm and a decrease in the “motility” (ability to move forward) of the sperm. This is in association with a decreased amount of testosterone that occurs with aging.
Erectile Function
While it seems that most people don’t know it, it is not necessary for a man to have an erection to experience orgasm and ejaculation. It is necessary, however, to have an erection if sexual intercourse is to take place.
An erection occurs, when under the influence of sexually arousing stimuli the penis becomes engorged with blood. An erection is a very complex biological phenomenon but it involves 2 chemicals that we can focus on that play a major role in both male and female sexual arousal. These are nitric oxide (NO) and cyclic guanosine monophosphate (cGMP). Both of these result in relaxation of smooth muscle that controls blood vessels within the penis. This results in increased blood flow within the penis and both of these chemicals are positively influenced by testosterone. That is, without sufficient testosterone, there will not be enough NO and cGMP to create an erection. It turns out that DHT (dihydrotestosterone) is the principle regulator of these chemicals and DHT is manufactured in the body from testosterone. This erection producing blood flow is 30 – 60 times the normal blood flow in the penis when it is soft. An alteration in blood flowing out of the penis traps 120 ml of blood in the erect penis. When flaccid, the blood pressure in the penis is about 10 – 15 mm Hg. When fully erect the pressure is over 120 mm Hg. After orgasm, under the influence of a hormone called oxytocin 2, the amount of cGMP declines rapidly. This results in constriction of the blood vessels that increased blood flow within the penis during erection. Then there is less blood flowing within the penis and together with an increased drainage of the entrapped blood the penis becomes flaccid (relaxed) again.
You can see the tissues of the penis that are affected during an erection in figure 2.

Erectile Dysfunction (ED)
There are many causes of erectile dysfunction. The most common reason involves changes in the blood vessels that lessen their ability to deliver blood to the penis. There can also be problems with the nervous system that interferes with the nerves that stimulate an erection. There can be problems due to certain drugs such as SSRI antidepressants, antihypertensives (blood pressure pills), anticholinergics, corticosteroids and others. There can also be hormone problems such as too much prolactin (a pituitary hormone) or low testosterone, the very common reason why we see men in the Masters Men’s Clinic.
Drugs such as Viagra, Cialis or Levitra act to maintain a high concentration of cGMP. These drugs have been a boon in treating erectile problems and work very well. However they are only successful about 60% of the time. They work only when a man is sexually excited. They do not help a man with low libido or low sexual desire. They have no effect whatsoever on the availability of testosterone. Since testosterone is necessary for the production and function of NO and cGMP, it appears that if the levels of testosterone are low, there is a good chance that Viagra, Cialis or Levitra won’t work very well. We have shown that for these “failures” it is possible to improve” around 50% of them with testosterone therapy. It turns out that the human penis needs more testosterone for its erectile function than was previously thought. It is quite acceptable to use these erectile medications plus testosterone replacement.
Viagra was the first of these drugs on the market. It should not be taken with food or alcohol. Typically it is effective within 30-60 minutes and it works for up to 8 hours. This does not mean that a man has an 8-hour erection. It means that if he is sexually excited anytime during those 8 hours, he probably will have a satisfactory erection. The usual dose is 50 to 100 mg.
Levitra is very similar to Viagra but it can be taken with food or alcohol. The usual dose is 10 to 20 mg. It is fast acting.
Cialis is a little different from the other two. It seems to take longer to work (45minutes to 3 hours) but it can have its effect over the following two to three days. This pill is known as “the weekender”.
Nocturnal and Morning Erections
Nocturnal erections (erections during sleep) occur during the REM (rapid eye movement) phase of sleep. These are about 7 times per night and occupy about 25% of the total sleep time in young men. The size of the erection is about 70% of an erection that is generated during healthy sexual arousal. In aging men, this drops to less than half (or sometimes not at all). Research shows that most dreams associated with nocturnal erections turn out not to be erotic in nature. Erections on waking, (morning erections) represent nocturnal erections associated with the last episode of REM sleep and are not related to bladder fullness. There really is no such thing as a “pee hard”. Testosterone is necessary for the existence of nocturnal erections and low levels of testosterone results in fewer of these erections. A reliable diagnostic sign that a man is low in testosterone is the loss of morning erections. When testosterone is supplemented, there is frequently a return of morning erections.
Male Sexual Function and the Brain
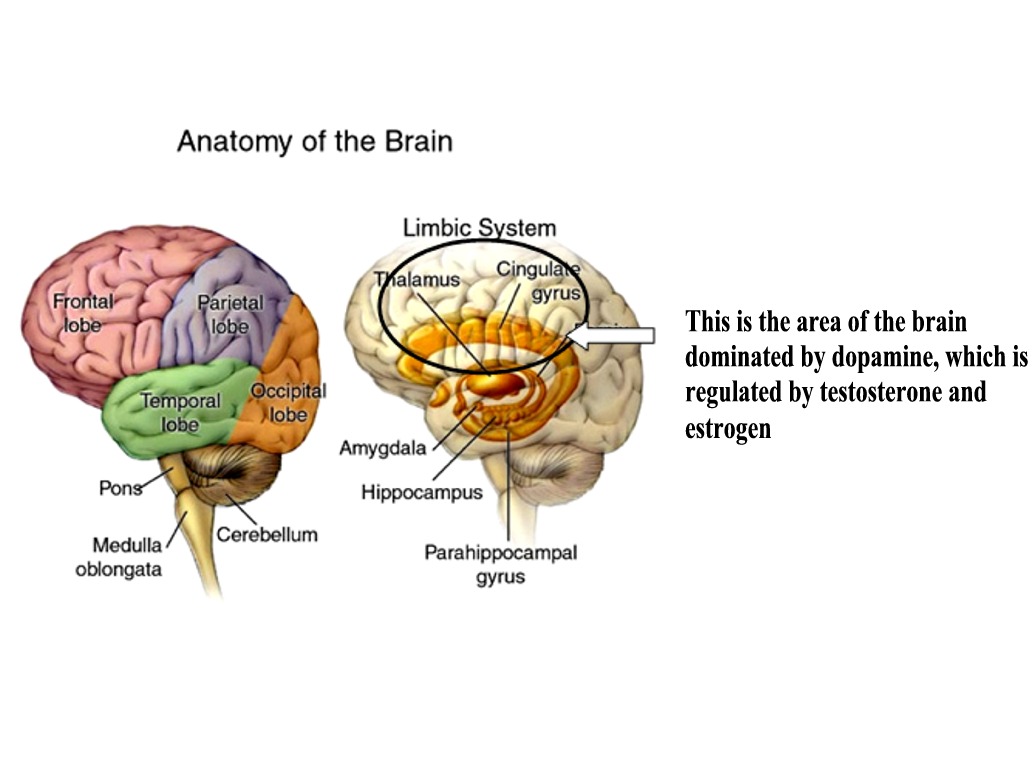
The brain is a major organ whose anatomy and function is regulated by testosterone, estrogen, progesterone and other hormones associated with the reproductive system.
All of our thought processes, bodily movements, and behaviours occur as a result of brain function. The brain works by the cells of the brain “talking” to each other. The brain’s cells produce chemicals that are exchanged with each other during this “talk”. One of these brain chemicals is dopamine, a chemical secreted by brain cells that plays a dominant role in mood and emotion. Dopamine is the principle “feel good” chemical of the brain and is particularly found in the “limbic” system of the brain that is the area that controls emotions. If dopamine signalling is reduced, there is a reduction in the reward or “feel good” value of everything. Dopamine rewards animals for doing things with survival value – eating or having sex, for example. Pleasure is involved in all types of decision-making, from choosing food to solving mathematical problems. Pleasure helps us plan our movements and allows our brains to filter and sort the mass of smells, sights, sounds and other information that bombard our senses. The dopamine system seems important for helping us to make the behavioural choices that will help us achieve the goals it has told us we desire 3,4,5.
Testosterone and estrogen play a major role regulating dopamine function. Good mental health is dependant upon healthy levels of testosterone. When levels of testosterone fall below optimal levels, men (and women too, for that matter) are more vulnerable to mood disorders such as depression.
There is a strong interrelationship between sexual function and mental health. Testosterone promotes the desire for sex and the chemical that sends the signal is dopamine. Orgasm further enhances dopamine and other brain chemicals that help with healthy brain function. Satisfactory sexual experiences also increase the production of testosterone that, as we have said, helps to regulate both brain and bodily function.
Research shows that when there are sexual problems, men are vulnerable to depression. As an example of the consequences of sexual dysfunction and mental health, studies have examined the relationship between erectile dysfunction (ED) and depression. These studies reveal that men with ED have high levels of depressive and anxiety symptoms. They also display considerable levels of anger and personality disorders. There is reduced quality of life, impaired social and job functioning and often substance abuse. Successful treatment of ED reverses much of such problems. In many men, part of the successful treatment involves testosterone therapy since in many men active testosterone levels will be low.
At the Masters Men’s Clinic we evaluate men for mood disorders as part of our routine investigation of suspected low testosterone. While very few men are referred to our clinic because of mood disturbance, it is striking that many men are suffering from mood disorders, particularly depression. When we treat these men with testosterone, it is remarkable to witness the vast improvement of these men back to good mental health (Figure 4).
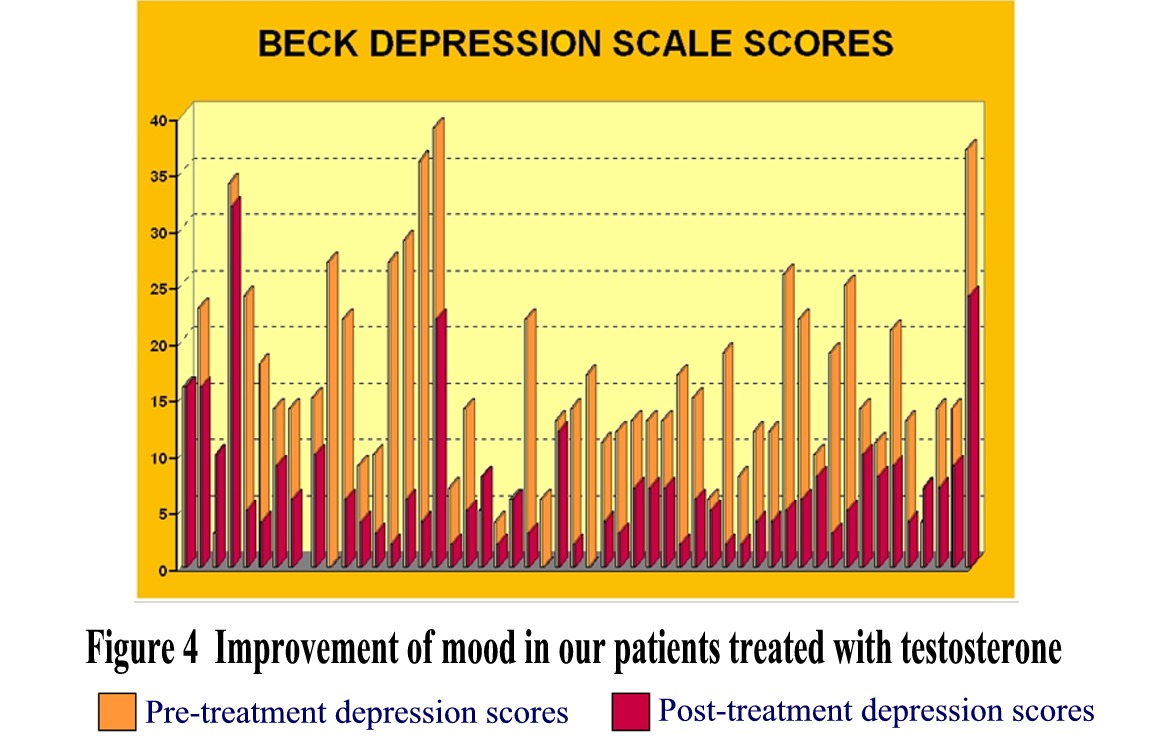
This figure shows the results of the first 50 of our patients at The Masters Men’s Clinic that were diagnosed with Andropause and treated with testosterone. These patients were not referred for depression but many had it. The yellow bars are their depression scores before treatment with testosterone and the red bars are their scores after 6 months of treatment with testosterone. Any score above 10 indicates some depressive disorder with higher values indicating more severe depression. As you can see, the vast majority of patients with depressed mood had it improved by testosterone therapy.
Male Sexual Functioning and Aging
Males reach peak sexual capacity in their late teens. With aging, a gradual decrease in sexual responsiveness occurs. It will take longer to achieve full erection. It will take more direct and intense genital stimulation to maintain an erection. Orgasms and the feeling of ejaculatory inevitability become less intense. Semen volume decreases with age, which means less orgasmic sensation. The penis becomes softer faster after sex and it takes much longer to regain another erection if it happens at all. The interest in having sex diminishes.
All of this happens at the same time that testosterone production and levels decrease. Testosterone production decreases with age because there is less LH (luteinizing hormone) from the pituitary to stimulate the testicular production of testosterone. In the testicles themselves, with age, there are either fewer or less responsive Leydig cells to produce testosterone. Further, there is also an increase in the concentration of a blood protein SHBG (sex hormone binding globulin) that binds testosterone and reduces the activity of testosterone that does exist. There is less tissue production of DHT that is critically necessary to full male sexual function and bodily well being. In addition, the testosterone receptors in the cells are less sensitive to even the same levels of testosterone.
There is also a substantial decrease in an adrenal hormone DHEA that provides some of the raw material from which testosterone is made. DHEA sensitizes cells to better utilize testosterone. If DHEA levels fall, there will be a reduction in testosterone activity that will result in all of the problems of low testosterone. Masters Men’s Clinic tests for DHEA levels and starts DHEA Replacement Therapy when needed.
For many men, there will also be an increased level of estrogen with age. This excess estrogen impacts on testosterone function that may result in many of the problems noted above. Master’s Men’s Clinic does test for increased estrogen levels and we do have excellent treatments for it.
CONCLUSION
Optimum testosterone levels are necessary for optimum sexual function. Testosterone levels that are low are easily improved with the current therapy at our clinic. No man with sexual problems should just accept them as part of aging or stress. He should be assessed by an expert in Andropause to see if low testosterone levels are the problem.
REFERENCES
1. Kandeel FR, Koussa VKT, Swerdloff RF • Male Sexual Function and Its Disorders • EndocrineReviews22(3):342–388
2. Lippert TH, Mueck AO, Seeger H, Pfaff A • Effects of Oxytocin Outside Pregnancy • Horm Res 2003; 60:262–271
3. Caldwell JD • A Sexual Arousability Model Involving Steroid Effects at the Plasma Membrane • Neuroscience and Biobehavioral Reviews September 2001
4. Gray et al. • Testosterone, Sexual Function, and Cognition • J Clin Endocrinol Metab, July 2005, 90 (7):3838 –3846
5. Pfaus JG • Neurobiology of sexual behaviour • Current Opinion in Neurobiology 1999, 9:751–758

