




CARDIOVASCULAR HEALTH AND TESTOSTERONE
Introduction
Men have larger bodies with more muscle mass and expend much more energy than women. There needs to be much more blood flow to the male body’s various systems and tissues to meet these physiological demands. This increased blood flow requires a strong heart and competent blood vessels capable of distributing this extra blood. Much has been learned about the cardiovascular effects of testosterone in the last few years and we know that testosterone plays a major role meeting this demand for extra blood flow.
The heart and blood vessels have a rich supply of testosterone receptors. These receptors are present in the aorta and peripheral blood vessels as well as in ventricular and atrial cells, including the normal male and female left ventricle.
Testosterone supplementation has shown beneficial effects with respect to the lipid profile (cholesterol and triglyceride levels), blood vessel and heart function.
For men, testosterone is necessary for a healthy cardiovascular system. Andropause, with its lower levels of testosterone, prevents optimal cardiovascular health.
Adverse Cardiac Effects of Testosterone Unsubstantiated
Experimental lowering of testosterone is associated with a decrease in heart weight and contractile function, which is corrected with testosterone replacement. 1
Research has clearly shown the effects of testosterone on the blood vessels, and they are beneficial. In the past, testosterone has been considered as one of the risk factors for coronary artery disease because men are more likely than women to show up in the doctor’s office with cardiovascular problems. The notion that normal levels of testosterone could cause atherosclerosis (hardening of the arteries) developed over many years and was accepted by many despite the complete lack of evidence supporting this idea. Curiously, a study of the biographies of great opera singers reported that the life expectancy of the castrati (boys castrated before puberty to maintain their beautiful high-pitched singing voices) was not different from intact male singers, a finding that supports the concept that testosterone does not have a negative effect on survival. 2
Indirect arguments have also been used to link testosterone and atherosclerosis, such as the fact that abdominal obesity seen in men could be influenced by sex hormones. Abdominal obesity is now recognized as a risk factor for coronary artery disease as part of the complex of metabolic abnormalities known as the Metabolic Syndrome. Similarly, the negative effects on blood fats reported with the abusive use of synthetic (17-alkylated) testosterone (used illegally by some athletes, body builders and weight lifters) are well known. However these effects do not apply to the bio-identical (the same as produced by the body) testosterone prescribed at the Masters Men’s Clinic.
The controversy about the effects of testosterone on atherosclerosis has been further stimulated by studies in animal models; Experiments on female monkeys fed a high fat diet showed that coronary atherosclerosis was more extensive in testosterone-treated animals than in untreated controls. However, in this same study, in spite of the more extensive atherosclerosis, testosterone reversed the decreased ability of the blood vessels to dilate and allow more blood flow, a major benefit.
Experiments conducted in the same animals showed that the combination of estrogen and testosterone increased total-body breakdown of LDL (bad cholesterol) to the same extent as estrogen alone. These finding would be consistent with a profile that would suggest a neutral or protective effect of testosterone. 3
Beneficial Effects of Testosterone in the Cardiovascular System
Recent studies have reported benefits such as a reduction in blood levels of triglycerides, LDL cholesterol, and reduction of central obesity (increased weight around the middle), which has been shown to be a risk factor in heart disease.
In addition, favourable changes have been reported in platelet aggregation (reduced formation of blood clots) and fibrinolytic activity (breakdown of blood clots), coronary vasomotion and exercise-induced heart ischemia (reduced blood flow). 4
Studies of large populations of men have shown that men with coronary heart disease have lower testosterone levels than normal controls. The serum levels of the adrenal androgen, dehydroepiandrosterone (DHEA), and its metabolite (DHEAS) decline more markedly in the aging male than do other sex hormones. The Massachusetts Male Aging Study assessed the levels of these in 1,709 men aged 40-79 years and correlated them with cardiovascular disease after controlling for other factors, such as serum lipid and hormone levels, smoking, alcohol intake, obesity, hypertension, diabetes mellitus, diet, medications, physical activity and psychological measures. Low serum DHEAS levels correlates strongly and independently with coronary artery disease (CAD). 5 Follow-up of the same population confirmed that both low DHEA and DHEAS predicted the development of CAD over a 9-year interval. 6 As well, plasma levels of DHEA are significantly decreased in men aged 26-40 years with a prior myocardial infarction (heart attack) compared with healthy men. 7 In X-ray studies of the heart (angiography), the lower the testosterone, the larger the extent of heart disease. 8,9
In the Multiple Risk Factor Intervention Trial (MRFIT) the changes in total testosterone were followed over 13 years. Decreases in testosterone levels with aging were associated with an increase in triglycerides and a decrease in HDL (good) cholesterol. 10
In fact, a number of studies have investigated the possible mechanisms by which testosterone may have a beneficial effect on the cardiovascular system. 11 Testosterone was found to relax coronary arteries and increase coronary flow. 12,13
Positive Effects of Testosterone on Coronary Arteries in Men with CAD
Human studies find significant blood vessel effects of testosterone. The intravenous administration of testosterone to men with CAD improved the function of the lining (endothelium) of the blood vessels. 14 As well, the administration of normal concentrations of testosterone induced coronary artery dilatation and increased coronary blood flow in men with established CAD. 15 Testosterone increased total exercise time and tolerance.
In addition, a study of low-dose testosterone in men with stable angina reported a significantly improved blood flow to the heart The magnitude of the benefit was proportionately greater in patients with lower plasma levels of testosterone. 16,17
Positive Effects of Testosterone on Lipid Profile
Other studies evaluated the effects of testosterone on lipids and lipoproteins. Testosterone replacement in hypogonadal men (men with low testosterone) and healthy elderly men caused a small decrease in total and LDL cholesterol without significant changes in HDL cholesterol. 18 This is a beneficial effect. Testosterone replacement resulted in a significant reduction in episodes of angina and a marked increase in blood flow to the heart. As well, treatment with testosterone shows a 12.5% reduction in total cholesterol, a 15% decrease in triglycerides and a 5% increase in HDL cholesterol after 3 months. 19 Once again these are beneficial effects. Another study showed that testosterone replacement in castrated animals inhibited early development of plaque (damage to the blood vessels) by a mechanism that involved the conversion of testosterone to estrogen by an enzyme present in the vascular wall. This finding provides an additional mechanism to explain the actions of testosterone in blood vessels. 20
Effect of Testosterone on Smooth Muscle In Blood Vessel Walls
Other studies have demonstrated that, in addition to the testosterone effects on the blood vessel lining, there are relaxing effects on the blood vessel smooth muscle. These effects are explained by an inhibition of calcium entry into the cells. This relaxation is also accomplished by testosterone helping potassium enter blood vessel cells.
The coronary arteries were found to be more sensitive to relaxation by testosterone than the aorta in both men and women. 21
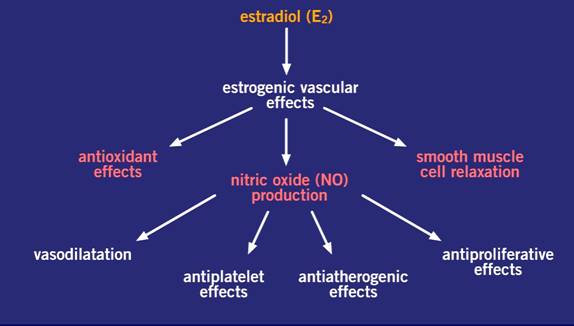
Part of the positive testosterone effects on a man’s cardiovascular system is due to the effects of the conversion of testosterone to estrogen by aromatase enzymes within the cardiovascular tissues. The two hormones, testosterone and estrogen, work together for positive effects. The graphic below lists the principle actions of estrogens.
Conclusion
In conclusion, contrary to the view that testosterone invariably has negative effects on the cardiovascular system, a view that was caused by the complications of illegal steroid abuse, recent evidence points to the beneficial effects of normal levels of testosterone. There is some indication that restoring normal healthy levels of testosterone may be helpful in preventing heart disease.
Cardiac patients should not be denied the benefits of physiologic testosterone replacement when there is clear indication for its use as there is no convincing clinical evidence that it is harmful.
The definitive role of testosterone replacement in the prevention of cardiovascular disease and the long-term implications of its use in cardiac patients must await further studies.
References
- Scheuer J, Malhotra A, Schaible TF, Capasso J. Effects of gonadectomy and hormonal replacement on rat hearts. Circ Res 1987;61:12-9.
- Nieschlag E, Nieschlag S, Behre HM. Lifespan and testosterone. Nature 1993;366:215.
- Wagner JD, Zhang L, Williams JK, Register TC, Ackerman DM, Wiita B, Clarkson TB, Adams MR. Esterified estrogens with and without methyltestosterone decrease arterial LDL metabolism in cynomolgus monkeys.
Arterioscler Thromb Vasc Biol 1996;16:1473-80. - Weidemann W, Hanke H. Cardiovascular effects of androgens. Cardiovasc Drug Rev 2002;20:175-98.
- Feldman HA, Johannes CB, McKinlay JB, Longcope C. Low dehydroepiandrosterone sulfate and heart disease in middle-aged men: Cross-sectional results from the Massachusetts Male Aging Study. Ann Epidemiol 1998;8:217-89.
- Feldman HA, Johannes CB, Araujo AB, Mohr BA, Longcope C, McKinlay JB. Low dehydroepiandrosterone and ischemic heart disease in middle-aged men: Prospective results from the Massachusetts Male Aging Study. Am J Epidemiol 2001;153:79-89.
- Slowinska-Srzednicka J, Zgliczynski S, Ciswicka-Sznajderman M, Srzednicki M, Soszynski P, Biernacka M, Woroszylska M, Ruzyllo W, Sadowski Z. Decreased plasma dehydroepiandrosterone sulfate and dihydrotestosterone concentrations in young men after myocardial infarction. Atherosclerosis 1989;79:197-203.
- English KM, Mandour O, Steeds RP, Diver MJ, Jones TH, Channer KS. Men with coronary artery disease have lower levels of androgens than men with normal coronary angiograms. Eur Heart J 2000;21:890-94.
- Phillips GB, Pinkernell BH, Jing TY. The association of hypotestosteronemia with coronary artery disease in men. Arterioscler Thromb 1994;14:701-6.
- Zmuda JM, Cauley JA, Kriska A, Glynn NW, Gutai JP, Kuller LH. Longitudinal relation between endogenous testosterone and cardiovascular disease risk factors in middle-aged men. A 13-year follow-up of former Multiple Risk Factor Intervention Trial participants. Am J Epidemiol 1997;146:609-17.
- Alexandersen P, Haarbo J, Byrjalsen I, Lawaetz H, Christiansen C. Natural androgens inhibit male atherosclerosis: A study in castrated, cholesterol-fed rabbits. Circ Res 1999;84:813-9.
- Yue P, Chatterjee K, Beale C, Poole-Wilson PA, Collins P. Testosterone relaxes rabbit coronary arteries and aorta. Circulation 1995;91:1154-60.
- Chou TM, Sudhir K, Hutchison SJ, Ko E, Amidion TM, Collins P, Chatterjee K. Testosterone induces dilation of canine coronary conductance and resistance arteries in vivo. Circulation 1996;94:2614-9.
- Ong PJ, Patrizi G, Chong WC, Webb CM, Hayward CS, Collins P. Testosterone enhances flow-mediated brachial artery reactivity in men with coronary artery disease. Am J Cardiol 2000;85:269-72.
- Webb CM, Adamson DL, de Zeigler D, Collins P. Effect of acute testosterone on myocardial ischemia in men with coronary artery disease. Am J Cardiol 1999;83:437-9,A9.
- Rosano GM, Leonardo F, Pagnotta P, Pelliccia F, Panina G, Cerquetani E, della Monica PL, Bonfigli B, Volpe M, Chierchia SL. Acute anti-ischemic effect of testosterone in men with coronary artery disease. Circulation 1999;99:1666-70.
- English KM, Steeds RP, Jones TH, Diver MJ, Channer KS. Low-dose transdermal testosterone therapy improves angina threshold in men with chronic stable angina: A randomized, double-blind, placebo-controlled study. Circulation 2000;102:1906-11.
- Zgliczynski S, Ossowski M, Slowinska-Srzednicka J, Brzezinska A, Zgliczynski W, Soszynski P, Chotkowska E, Srzednicki M, Sadowski Z. Effect of testosterone replacement therapy on lipids and lipoproteins in hypogonadal and elderly men. Atherosclerosis 1996;121:35-43.
- Rosano GM, Mercuro, G et al. Antianginal and lipid-lowering effects of chronic oral androgen supplementation in elderly male patients with coronary heart disease. J Am Coll Cardiol 2001;37:254A.
- Nathan L, Shi W, Dinh H, Mukherjee TK, Wang X, Lusis AJ, Chaudhuri G. Testosterone inhibits early atherogenesis by conversion to estradiol: Critical role of aromatase. Proc Natl Acad Sci USA 2001;98:3589-93.
- Yue P, Chatterjee K, Beale C, Poole-Wilson PA, Collins P. Testosterone relaxes rabbit coronary arteries and aorta. Circulation 1995;91:1154-60.

