




ANDROPAUSE, TESTOSTERONE AND THE PROSTATE GLAND
Introduction
The prostate gland is a walnut sized gland in the male reproductive system just below the bladder that supplies fluid for the sperm during ejaculation.
As men age the prostate gland tends to enlarge, producing a condition called benign prostatic hypertrophy (BPH). Also, the incidence of prostate cancer increases. These two events happen at a time in a man’s life when his testosterone levels are falling. This seems a little puzzling, since it is well known that testosterone stimulates prostate growth and the growth of an existent cancer of the prostate. Obviously there are factors other than testosterone at work to cause the prostate to enlarge and in the initiation of prostate cancer. Because of testosterone’s stimulatory effect on prostate tissue, the physician and the patient must be vigilant monitoring possible changes within the prostate gland in a man being treated with testosterone.
Prostate Anatomy, Growth and Function
The prostate gland is a vital part of the male reproductive system. It’s amazing that today most men know precious little about this gland that does so much for them.
A newborn male’s prostate is very small about the size of a grain of wheat. The prostate remains very small until puberty. At the onset of puberty it begins to grow dramatically until around the age of twenty.
A healthy adult prostate weighs about 20 – 25 grams (2/3 to 3/4 of an ounce). It is walnut shaped and it measures 4 x 2 x 3 centimeters (1.6 x 1 x 1.2 inches). It is divided into 2 lobes. It contains smooth muscle cells capable of contracting to expel the prostatic fluid.
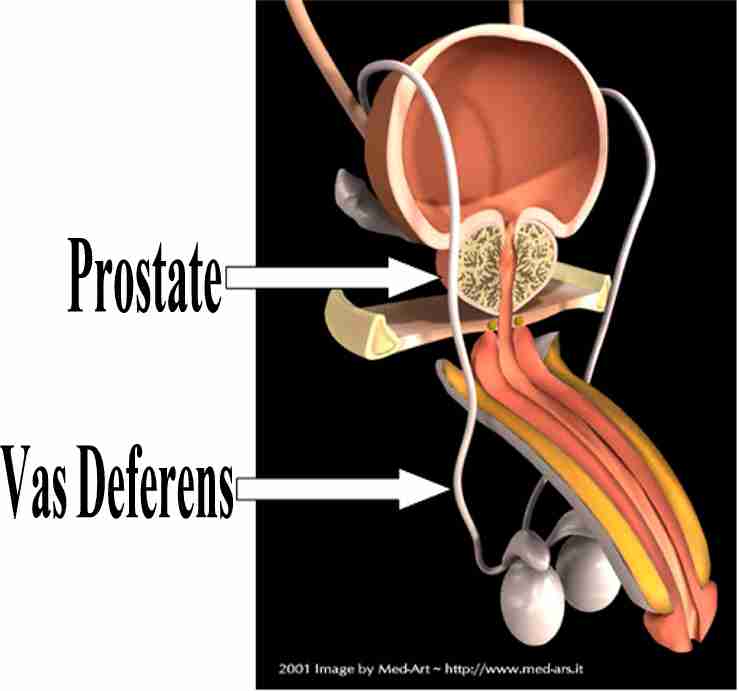
As you can see from the illustration below, the prostate surrounds the urethra, which carries urine from the bladder to the penis.

The seminal vesicles attach to the prostate and produce secretions that mix with prostatic fluid to form semen.

Graphics courtesy of
www.med-ars.it
The tubes (Vas Deferens) from the testicles carry sperm to the prostate where the sperm are mixed with the prostate and seminal vesicle fluid. The fluid (semen) is ejaculated during orgasm by a connection to the urethra called the ejaculatory ducts. Normal ejaculation produces about 3 – 5 cc (teaspoon) of semen.. The sperm makes up less than 1% of this volume with the seminal vesicles and the prostate producing the remainder of the volume. The prostate, which is made up of thousands of fluid-producing glands, itself secretes 25 – 35% of the total fluid volume. It is during high arousal in particular, that the prostate secretes this fluid. If extended arousal is not followed by ejaculation, the prostate can become tender and somewhat sore. This condition seems to account for what some call “blue balls”. The ejaculate is slightly acidic (pH 6.5) and contains proteins, hormones, growth factors, lipids, zinc, potassium, citric acid, fructose, prostaglandins etc.
The prostate is divided into three zones: a central zone, a peripheral zone, which occupies some 70% of the prostate’s volume, and the transitional zone between the peripheral zone and the central zone. The peripheral zone is the most common site of prostate cancer and the transitional zone is the exclusive site of benign prostatic hyperplasia (BPH). It is the peripheral zone that a doctor can feel by a finger in the rectum. The central zone is involved with the connection of seminal vesicles to the prostate and is rarely associated with any disease process.
The size of the prostate is normally fairly constant until the forties. Then, due to hormone changes, the prostate begins to bulk up. This later development and function of the gland are primarily dependent on hormone derivatives of testosterone called DHT (dihydrotestosterone) and estrogens.
Prostate-Specific Antigen
There are many prostatic secretory proteins. In particular we are interested in prostate-specific antigen (PSA). PSA helps to liquefying the ejaculate. Without it, men would ejaculate jellybean-sized globs. Clinically, it is a valuable marker for the detection of prostate cancer and for following response to treatment. PSA density (total PSA/volume of the prostate gland) and velocity (changes in PSA over time) are useful in differentiating benign prostate hyperplasia (BPH) from prostate cancer.
Andropause, Prostate Disease and Testosterone Supplementation in Men
Andropause is a situation associated with low levels of testosterone. Symptoms of Andropause are any combination of the following: fatigue, poor sleep, general aches and pains, forgetfulness, reduced interest in sex, poor ejaculation and poor mood. Andropause can be improved with testosterone replacement therapy (TRT).
A concern of testosterone supplementation is that it will lead to the development or progression of prostate diseases such as BPH and prostate cancer. Both conditions do not develop without exposure to testosterone. Testosterone itself does not cause BPH or prostate cancer, but rather testosterone together with several other factors can combine to cause these problems.
Testosterone Replacement Therapy (TRT) and Prostate Safety
Testosterone replacement therapy (TRT) in a man with low testosterone may result in a slight and usually insignificant increase in the volume of the prostate gland. This means that there will be little effect on the PSA levels and the ability to urinate. When it comes to prostate cancer, there is no evidence that testosterone replacement promotes development of prostate cancer; however, an existing cancer may grow from testosterone therapy. 1
Benign Prostatic Hypertrophy (BPH)
The development of BPH is caused by DHT (dihydrotestosterone) 2 along with the actions of estrogens. 3 After 40 the growth of the prostate is uneven. It is concentrated in the transition zone next to the urethra. This can, for some men, squeeze the urethra enough to cause problems with urinating (hesitancy).
Prostate size increases with age in normal men but not in men with low levels of testosterone. When testosterone deficient men are treated, the prostate volume increases but only to the size expected for men with normal levels of testosterone of the same age. 4 Many studies have shown no effect of testosterone replacement on PSA or prostate volume. 5 We would not give testosterone to a man with severe bladder obstruction due to an enlarged prostate but we have given testosterone therapy to some men with moderate symptoms of a poor urine stream. The physician must use good clinical judgment and monitor closely for any possible detrimental effects; however, the benefits of TRT should not be denied outright because of the presence of mild, stable symptoms of reduced urine flow (obstruction). 6

Prostate Cancer
Testosterone therapy should not be given to men suspected of having prostate cancer. This includes men with an abnormal digital rectal exam (DRE) or PSA for whom the diagnosis of cancer has not been ruled out, and those recently treated for prostate cancer in which both the DRE and PSA are normal. After a prudent period (perhaps 2 or 3 years) without evidence of a recurrence of their cancer, the pros and cons of testosterone therapy should be carefully considered and the restriction could be lifted. It is necessary to stress that these men must be monitored closely within the first 2 years of the onset of testosterone therapy, when regrowth of the cancer is most likely to occur. 7
Role of Other Factors in the Development of Prostate Cancer
Currently, the evidence does not support the notion that normal levels of testosterone are associated with increased risk of prostate cancer. Other factors (environmental, genetic) are likely to be very significant.
Studies suggest that obesity can be a risk for prostate cancer 8 and that dietary factors either directly or through the action of sex hormones may have an important bearing on the development of prostate cancer. 9 Saturated fat (found in red meat, etc) consumption is associated with increased risk of prostate cancer: the greater the consumption the higher the risk.
Practical Suggestions for Prostate Safety – Before and During Treatment with Testosterone
Before each man is started on testosterone replacement therapy (TRT) he must have a normal digital rectal examination (DRE) and a PSA below 4.0
If the PSA has increased more than 0.75 units in the last 6 months this should be investigated before treatment starts.
In our clinic we test the following before treatment: testosterone, haematocrit, cholesterol, thyroid, liver enzymes, LH, estradiol, prolactin, DHEA, fasting glucose and insulin.
After testosterone replacement therapy (TRT) has started we recheck these tests at intervals of 4 months, 6 months and 12 months and then twice a year thereafter.
Conclusion
The main concern regarding testosterone administration to an aging man relates to prostate safety. The careful clinician using good judgment and having sufficient knowledge should feel confident in using testosterone therapy in well-screened symptomatic men. Careful follow-up and adherence to available recommendations 10 are essential.
References
1. Huggins C, Hodges CV. The effect of castration, of estrogen and androgen injection on serum phosphates in metastatic carcinoma of the prostate. Cancer Res 1941;1:293.
2. Meikle AW, Stephenson RA, Lewis CM, Middleton RG. Effects of age and sex hormones on transition and peripheral zone volumes of prostate and benign prostatic hyperplasia in twins. J Clin Endocrinol Metab 1997;82:571-5.
3. Thomas JA, Keenan EJ. Effects of estrogens on the prostate. J Androl 1994;15:97-9.
4. Behre HM, Bohmeyer J, Nieschlag E. Prostate volume in testosterone-treated and untreated hypogonadal men in comparison to age-matched controls. Clin Endocrinol 1994;40:341-9.
5. Tenover JS. Androgen administration to aging men. Endocrinol Metab Clin North Am 1994;23:877-92.
6. Wang C, Swerdloff RS. Should the nonaromatizable androgen dihydrostersosterone be considered as an alternative to testosterone in the treatment of andropause? J Clin Endocrinol Metab 2002;87:1462-6.
7. Morales A. Testosterone and prostate safety. Europ Urology 2002;37:1-6.
8. Andersson SO, Wolk A, Bergström R, Adami HO, Engholm G, Englund A, Nyrén O. Body size and prostate cancer: A 20-year follow-up study among 135006 Swedish construction workers. J Natl Cancer Inst 1997;89:385-9.
9. Ross RK, Henderson BE. Do diet and androgens alter prostate cancer risk via a common etiological pathway? J Natl Cancer Inst 1994;86:252-4.
10. Morales A, Lunenfeld B. Investigation, treatment and monitoring of late-onset hypogonadism in males: Official Recommendations of ISSAM. Aging Male 2002;5:74-86.

